
Rotator Cuff Related Shoulder Pain: Understanding Shoulder Pain Beyond “Impingement”
Shoulder pain is one of the most common musculoskeletal presentations seen in physiotherapy, particularly in active individuals, overhead athletes, swimmers, gym-goers, and manual workers. One of the most common diagnoses within this group is Rotator Cuff Related Shoulder Pain (RCRSP).
Historically, shoulder pain was often labelled as “impingement”, with the idea that structures within the shoulder were being mechanically pinched during movement. More recent research has challenged this model, with current evidence suggesting shoulder pain is far more complex and influenced by factors including tissue capacity, loading patterns, movement variability, sensitisation, recovery, and overall conditioning.
Importantly, the presence of pain does not necessarily mean significant structural damage.
What is the rotator cuff?
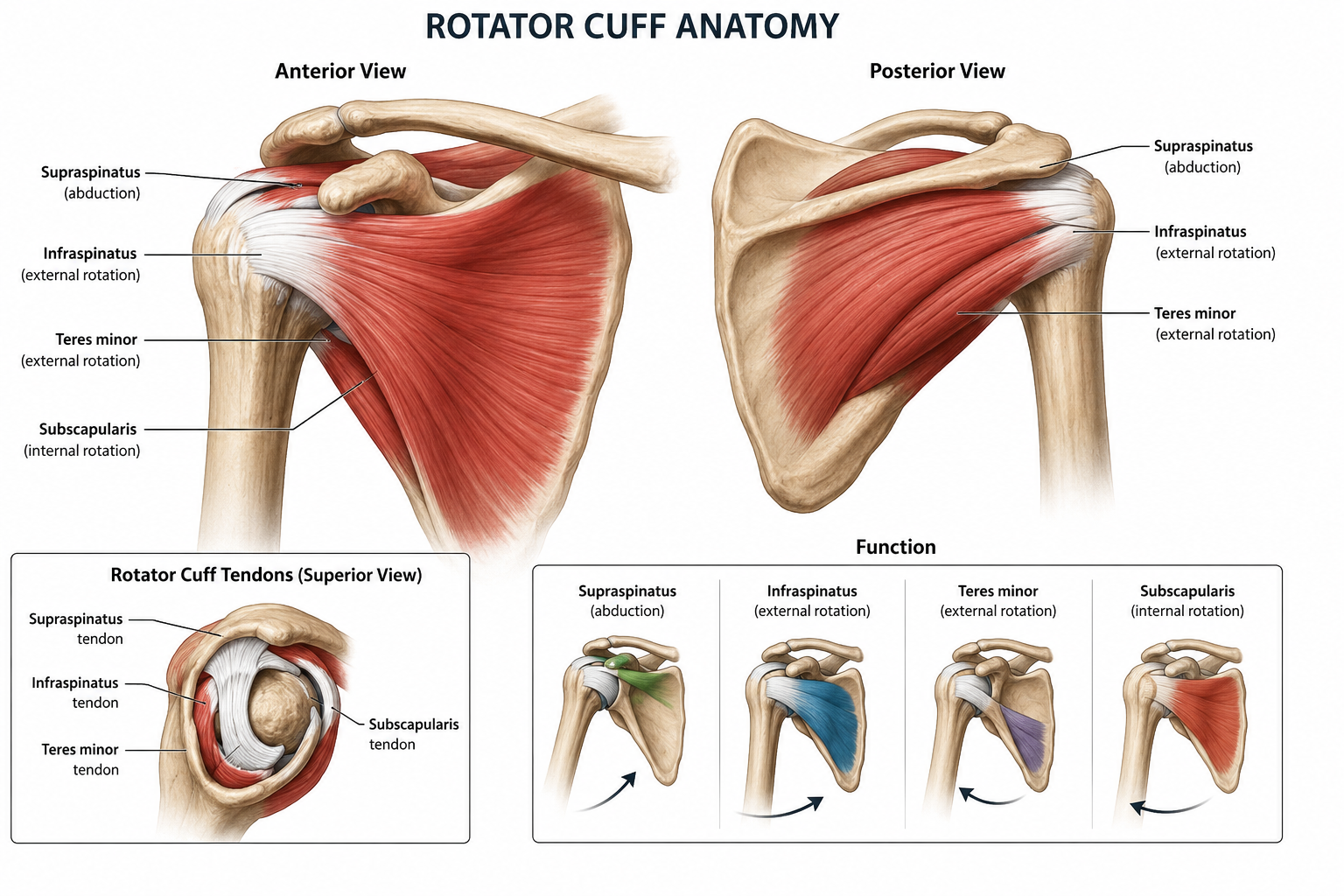
The rotator cuff consists of four muscles:
Supraspinatus
Infraspinatus
Teres minor
Subscapularis
These muscles help stabilise the glenohumeral joint and contribute to force production and dynamic shoulder control during movement.
The shoulder sacrifices stability for mobility. As a result, the rotator cuff plays a significant role in maintaining efficient shoulder mechanics during both sporting and everyday activities.
What is Rotator Cuff Related Shoulder Pain (RCRSP)?
RCRSP is an umbrella term encompassing a range of clinical presentations involving the rotator cuff tendons and associated structures.
This may include:
Rotator cuff tendinopathy
Reactive tendon pain
Subacromial pain syndrome
Bursal irritation associated with cuff overload
Partial thickness rotator cuff pathology
Importantly, structural findings on imaging often correlate poorly with symptoms.
Numerous studies have demonstrated high rates of asymptomatic findings on MRI and ultrasound, including tendon degeneration, bursitis, and partial thickness tears in pain-free individuals, particularly with increasing age.
This means imaging findings should always be interpreted within the context of the individual clinical presentation rather than assumed to be the direct cause of pain.
Common symptoms
Individuals with RCRSP commonly report:
Pain with overhead activity
Pain during pressing or lifting movements
Pain lying on the affected shoulder
Pain with reaching away from the body
Reduced confidence loading the shoulder
Pain during swimming or throwing
Temporary reductions in strength secondary to pain inhibition
Symptoms are often aggravated following spikes in load or volume rather than from a single identifiable traumatic event.
Why does shoulder pain develop?
Current evidence supports the concept that tendon pain often develops when the applied load exceeds the tissue’s current capacity to tolerate it.
Common contributing factors may include:
Rapid increases in training volume or intensity
Sudden increases in overhead loading
Reduced rotator cuff strength or endurance
Deconditioning
Poor recovery or sleep
High cumulative workload
Psychosocial stressors
Previous shoulder injury history
This does not mean there is always a single “root cause” or biomechanical fault driving symptoms. Human movement is highly variable, and pain is multifactorial.
While factors such as scapular mechanics, thoracic mobility, or shoulder strength may contribute in some individuals, they should not be viewed in isolation or interpreted as definitive causes of pain.
Is it really “impingement”?
The term “shoulder impingement” has become increasingly controversial within musculoskeletal practice.
While compression of structures within the subacromial space can occur physiologically during movement, research has shown that many individuals with narrowed subacromial spaces have no pain, while others with pain demonstrate minimal structural abnormality.
Current understanding suggests symptoms are more likely related to a combination of:
Rotator cuff load tolerance
Tendon sensitivity
Local tissue irritability
Strength and conditioning deficits
Central and peripheral sensitisation mechanisms
This distinction is important because language matters. Telling someone their shoulder is “pinching” or “wearing out” can increase fear, reduce confidence with movement, and negatively impact recovery.
Physiotherapy management
Management of RCRSP is typically centred around progressive loading and exercise-based rehabilitation.
At SurfEdge, rehabilitation is individualised based on the person’s goals, training demands, irritability levels, and functional limitations.
Management may include:
Graduated rotator cuff strengthening
Isometric loading strategies in irritable presentations
Progressive overhead loading
Kinetic chain and scapular strengthening where appropriate
Thoracic mobility interventions if relevant
Gym and sport-specific rehabilitation
Education regarding load management and symptom response
Return to sport planning
Manual therapy may be used adjunctively in some cases to assist short-term symptom modulation or improve movement tolerance, however exercise and progressive loading remain the cornerstone of long-term management.
Should you stop training?
Complete rest is rarely optimal.
Prolonged unloading may reduce tissue capacity further and contribute to deconditioning. Instead, rehabilitation generally aims to identify an acceptable loading range where the shoulder can continue to tolerate movement while symptoms gradually settle.
In many cases, temporary modification of aggravating activities is more appropriate than complete cessation.
This may involve temporarily reducing:
Overhead pressing volume
Swimming load
Throwing frequency
Training intensity
Repetitive overhead occupational tasks
Pain during rehabilitation is not always harmful, and some level of tolerable symptom response during exercise can be acceptable depending on the individual presentation.
What does rehabilitation look like?
Rehabilitation is typically staged and progressive.
Early Stage
Focus may include:
Pain modulation
Isometric loading
Maintaining shoulder movement
Gradual reintroduction to tolerated loading
Mid Stage
Focus generally progresses toward:
Rotator cuff strengthening
Improved load tolerance
Scapular and kinetic chain integration
Progressive resistance training
Late Stage
Rehabilitation becomes increasingly specific to the individual’s functional goals, including:
Overhead strength and endurance
Plyometric or power-based loading
Return to swimming or throwing programs
Sport-specific conditioning
The overall goal is not simply reducing pain, but improving the shoulder’s ability to tolerate the demands placed upon it long term.
When should you seek assessment?
Assessment is recommended if:
Shoulder pain persists beyond several weeks
Symptoms are limiting work, sport, or sleep
You are losing strength or function
Symptoms repeatedly recur
You are unsure how to safely continue training
Early management can help guide appropriate loading and reduce the likelihood of symptoms becoming more persistent.
Final thoughts
Rotator cuff related shoulder pain is common, particularly in active populations, but the presence of pain does not automatically indicate significant structural damage.
Modern physiotherapy management focuses less on “fixing” posture or correcting isolated biomechanical faults, and more on improving load tolerance, restoring confidence with movement, and progressively rebuilding shoulder capacity.
With an appropriately structured rehabilitation program, most individuals can successfully return to training, sport, and normal daily function without requiring surgery or prolonged rest. For more information about the shoulder conditions we treat, click HERE
If shoulder pain is limiting your training, work, sleep, or performance, early assessment and appropriate rehabilitation can make a significant difference. At SurfEdge Sports Physiotherapy, we take an evidence-based approach to shoulder rehabilitation, focusing on identifying contributing factors, improving load tolerance, and helping you return confidently to the activities that matter most to you.
Whether you are dealing with persistent gym-related shoulder pain, swimming-related symptoms, overhead sporting demands, or recurrent rotator cuff irritation, physiotherapy can help guide an appropriate recovery plan tailored to your goals.