
Bone Stress Injuries in Elite Female Athletes - Why it’s rarely just a bone problem
Bone stress injuries are one of the most common and frustrating injuries I see in high-level female athletes, particularly in endurance and surf life saving environments. They’re disruptive, they take time, and more often than not, they don’t come out of nowhere.
What I’ve learnt clinically is that if you only treat the bone, you will keep missing the point. A bone stress injury is not just a local tissue overload. It’s usually the end result of a system that’s not coping with the demands being placed on it.
At a basic level, bone stress injuries occur when the rate of bone breakdown exceeds the rate of bone repair. Under normal circumstances, bone is constantly remodelling in response to load. That’s how we get stronger. But when the balance tips, whether due to excessive load, inadequate recovery, or underlying physiological factors, the bone starts to fail along a continuum from stress reaction through to fracture.

In female athletes, that imbalance is very rarely explained by training load alone. This is where the conversation needs to shift toward energy availability and the broader concepts of RED-S and the female athlete triad.
The female athlete triad has traditionally been described as the interaction between low energy availability, menstrual dysfunction, and low bone mineral density. While that framework is still useful, it doesn’t capture the full picture we see in practice.
RED-S, or Relative Energy Deficiency in Sport, expands on this. It recognises that low energy availability affects multiple systems, not just reproductive and bone health, but also metabolism, recovery, immune function, and ultimately performance. And importantly, athletes don’t need to present with all the classic signs to be at risk.
Low energy availability sits at the centre of this.
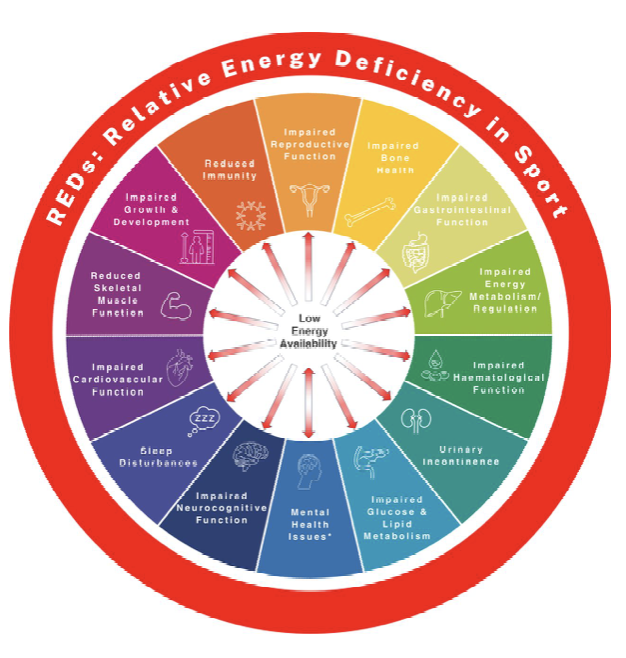
RED-S is multifactorial, with no one contributing factor explaining the condition, but rather the interplay between multiple contributors
If an athlete is not taking in enough energy to support both their training load and basic physiological function, the body starts to prioritise. Processes like reproduction and bone formation are effectively downregulated. Hormonal changes follow, particularly reductions in oestrogen, which plays a key role in maintaining bone health. The result is a system that is less resilient to load.
What makes this tricky is that it’s often not obvious. These athletes are still training, still competing, and often still performing at a high level. They might not report disordered eating. Their menstrual cycle might be irregular rather than absent. It’s subtle, and it’s easy to miss if you’re only looking at the injury in isolation.
From a loading perspective, these athletes are also operating close to the edge.
High training volumes, competition demands, travel, and inconsistent fuelling all accumulate. What might be a tolerable load in a well-fuelled, well-recovered athlete becomes excessive in someone who is under-resourced. Add in biomechanical factors, such as reduced calf capacity, poor lumbopelvic control, or inefficient load transfer, and you have the perfect setup for a bone stress injury.
Clinically, there are usually warning signs. Recurrent bone stress injuries, delayed healing, persistent fatigue, changes in menstrual patterns, or a history of multiple injuries across different sites should all raise concern. These are not just unlucky athletes. There is almost always something underpinning it.
Management, in my experience, only works when you address both the load and the system. Offloading is important, but complete rest is rarely the answer unless you’re dealing with a high-risk injury. Most athletes need a reduction and modification of load rather than removal of it, along with maintaining some level of conditioning. But unless energy availability is addressed, you’re just buying time.
Increasing overall energy intake, improving fuelling around training, and often involving a sports dietitian is critical. This is not something that resolves with a generic “eat more” approach. It needs to be structured and, in many cases, supported.
Hormonal health also needs to be considered properly. Masking the issue with hormonal contraception doesn’t fix the underlying problem. The goal should always be restoration of normal physiological function, which may require input from a sports physician.
Rehabilitation itself needs to be progressive and objective. It’s not just about settling symptoms. It’s about rebuilding capacity. That means addressing strength deficits, particularly through the calf, hip, and trunk, and reintroducing impact in a staged way.
More importantly, it means actually training the bone.
Heavy resistance work and appropriately progressed plyometrics are essential if you want to improve bone capacity. If you only ever work in low-load environments, you’re not giving the bone the stimulus it needs to adapt. One of the biggest challenges in this space is that it’s rarely straightforward.
Not every athlete presents clearly. Some have regular menstrual cycles but still demonstrate signs of low energy availability. Others appear healthy on the surface but repeatedly break down. High performers, in particular, are very good at masking underlying fatigue and dysfunction.
This is where ongoing monitoring and a multidisciplinary approach become important. As physios, we play a central role, but we shouldn’t be managing this in isolation.
Ultimately, bone stress injuries in female athletes are not just about managing load. They are about understanding whether the athlete has the capacity to tolerate that load in the first place. If that piece is missed, the cycle tends to repeat. And in my experience, the question we should be asking isn’t whether the athlete is doing too much. It’s whether their body has enough to support what they’re asking of it.
At the end of the day, bone stress injuries in female athletes are rarely just about how much they’re training. They’re about whether the athlete has the physiological capacity to support that training. If we don’t address energy availability, hormonal health, and overall system load, we might get them back in the short term, but we haven’t actually changed anything. The goal isn’t just to get an athlete through the current injury, it’s to build a body that can consistently tolerate high performance demands without breaking down. If you’re dealing with a stress fracture, recurrent bone stress injuries, or an athlete who just isn’t progressing, book in and we’ll look at the full picture, not just the injury.